Thyroid and Lipedema Diseases: Life Out of Balance – Part 2
As we discussed in the previous article life is about balance. When your life or your body is out of balance it opens the door to disease and chronic conditions, among those are thyroid conditions and diseases. Unfortunately, the prevalence of thyroid conditions is rapidly on the rise and if you are experiencing any of the symptoms listed in the previous article then you should strongly consider having your thyroid function fully evaluated by an Endocrinologist or a qualified Naturopath.
Once you have your results in hand from a FULL thyroid panel of tests and FULL supporting vitamins and minerals tests, you will need to understand what is happening within your body and if any thyroid disease or condition is present. The following is an overview of the most common diseases and conditions along with situations that may indicate thyroid problems but in actuality be caused by a related underlying condition.
Remember, you are a partner with your doctor and need to fully understand what is making you feel sick. Educate yourself the best you can so you can have meaningful conversations about test interpretations and a possible diagnose. Both of you are trying to achieve the same thing – your improved health!
Diagnosing Thyroid Conditions and Diseases
Diagnosing thyroid conditions and diseases is a combination of a comprehensive blood panel review PLUS a list of your current or worsening symptoms. It may also involve an ultrasound or fine needle aspiration (FNA) if a goiter, nodules or cancer is suspected. And don’t forget to share any family history of thyroid issues as genetics does play a factor in your analysis.
It should be noted that blood tests represent a snapshot in time and can fluctuate throughout the day. It is also limited to the hormones, minerals, vitamins and proteins floating in your bloodstream and does not indicate how your body is utilizing each of them. This is why symptomology is an important factor in your diagnosis.
Understanding Your Test Results

There are acceptable levels or test ranges for each test performed, usually determined by labs based on the prevalence of the population being served. The acceptable levels are based on a population of people with healthy thyroid function and no known metabolic issues. These established levels are usually in a standard unit of measure so you can compare results over time.
Unfortunately, the levels, ranges and units of measure vary from country to country and even between healthcare and lab organizations. Some countries have more restricted levels and ranges before medical professionals decide to apply treatment. We will be looking mostly at the levels and ranges within the United States in this article.
Acceptable versus Optimal Levels
Acceptable test levels and ranges will usually present as a green bar in your report with a specific value over top and a yellow bar on either side to indicate high or low values. (Note, color combinations and presentation may vary from country to country and even between healthcare and lab organizations within the United States.) You will also see the units of measure and perhaps some guidelines under the bar or value.
What you will not see is the “optimal” level for each test result. This value represents the level an average adult should strive to achieve that allows you to feel your best. Your medical professional should be able to give you this value. (Note: optimal levels may vary for children, pregnant women and those who had cancer treatment.) It is entirely possible to be within the “normal” test range and still not feel well until you move into the “optimal” range. It should also be noted some people may not feel well despite being in the optimal range. It is only a target number.
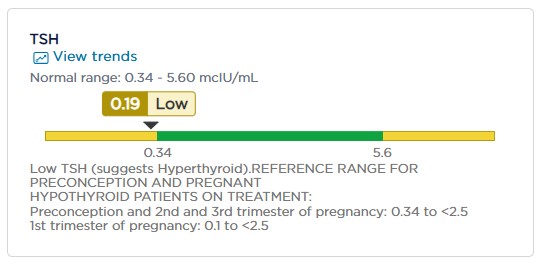
The image above is one of my recent thyroid labs test results for TSH (thyroid stimulating hormone). You will notice my levels are outside the normal range (in green) and marked low. There is a note below with a generic observation that levels below normal are indicative of hyperthyroidism. However, I am NOT hyperthyroid. This one test, which many Endocrinologists favor as the preferred thyroid health marker, cannot tell you the FULL story of my thyroid health without the levels of the other tests in the panel.
Understanding Your Thyroid Test Results
This is a sample thyroid test panel with both reference and optimal ranges listed. Again, these ranges may vary from lab to lab, between healthcare organizations and even between countries, especially the TSH levels. These are dependent on factors such as ethnicity, if you live in iodine deficient areas, standard dietary habits and economic development areas.
| Test Name | Reference Range | Optimal Range |
| TSH | 0.4 – 5.0 mlU/L | 1.0 – 2.0 mlU/L |
| Total T3 | 0.8 – 2.0 ng/ml 60 – 181 ng/dl | 0.8 – 2.0 ng/ml |
| Total T4 | 4.5 – 9.8 ug/dl | 4.5 – 9.8 ug/dl |
| Free T3 | 2.8 – 4.0 pg/ml | 3.0 – 4.0 mlU/L |
| Free T4 | 0.89 – 1.76 ng/dl | 1.0 – 1.17 mlU/L |
| Reverse T3 | 5.0 – 25.0 ng/dl | Less than 15 ng/dl |
| TPO Antibodies | Below 35 IU/ml | Below 35 IU/ml |
Optimal levels are desired but only if your symptomology supports your optimal level findings. It is nearly impossible for people to have optimal ranges in all measurements. Again, these are guidelines to shoot for and do not necessarily mean you are “cured” or will automatically have your symptoms abated.
Diagnosing Your Condition
Now that you have all your test results, what does it all mean? Your doctor, most likely an Endocrinologist or Naturopath, will review all your test results, family history and your symptomology to diagnose your condition. Below is a general guide to identifying which condition your tests and symptomology may suggest. It does not represent all the nuances that may influence the diagnosis of one condition over another. (1)
| Condition | TSH | T3/T4 | TPO Antibodies |
| Hypothyroidism | Elevated (Usually greater than 2.0) | Low (Usually in the bottom 20-25% of the range) | Normal or not present |
| Hashimoto’s Disease | Elevated but could fluctuate in normal range | Low (Usually in the bottom 20-25% of the range) | Elevated |
| Graves Disease | Low (Usually close to 0) | T3 is high FT4 may be low | Elevated |
| Hyperthyroidism | Low (Usually lower than 0.4) | T3 is high T4 is high | Normal or not present |
There are situations such as the presence of thyroid nodules that may stimulate the overproduction of T4 hormone suggesting on the surface you may have hyperthyroidism. However, when the nodules are treated or removed the situation resolves and you may be back to being euthyroid, meaning having a normal thyroid with normal thyroid hormone function.
You may also have a situation where your reverse T3, rT3, is abnormally high, which may lower your T4 and T3 hormone numbers. Normal T4 hormone function cleaves an iodine atom from its outer ring, converting it to the active T3 hormone through a deiodinase enzyme process. However, if the body sends a signal it is suffering an illness or injury, or there is significant caloric reduction, the T4 hormone will convert to the inactive rT3 creating an energy conservation mode. Metabolism is slowed and the amount of T3 entering your cells is reduced making you feel fatigued. (Your body doesn’t need a bunch of energy when it is down trying to heal.) Once your illness is resolved or you resume eating healthy caloric meals, your rT3 hormones should return to an acceptable level and normal T4 to T3 conversion will resume.
Impacts of Vitamins and Minerals
As you just read, there are situations where thyroid function and hormone production can appear to be impaired by a disease or condition but are actually impacted by something else that can be readily corrected. This can be the case for any abnormal vitamin or mineral tests. These vitamins and minerals are essential to thyroid function, hormone production, conversion, transport and cellular activity.
Abnormalities in these key vitamins and minerals. specifically deficiencies, can impact the overall operation of your thyroid function within the body and begin to generate true thyroid conditions and diseases.
- Iodine – the key building block of T4 and T3 hormones
- Selenium – critical for converting T4 to the active T3 hormone
- Zinc – helps regulate thyroid hormones
- Iron – also necessary for the conversion of T4 to the active T3 hormone
- Magnesium – aids in the conversion process
- B Vitamins (B12, B9, B2) – essential for overall metabolism, hormone synthesis, and healthy function of the nervous system
- Vitamin A (retinol) – facilitates the activation of receptors within the cells, facilitates conversion of T4 to T3 hormone, impact the pituitary gland’s ability to synthesize and secrete TSH
- Vitamin D – immune system function and preventing autoimmune thyroid diseases
- Vitamin C – support overall thyroid function and reduce oxidative stress
- Vitamin E – helps in immune function and metabolic processes (2)

The above test result illustrates a vitamin A deficiency, specifically retinol, which is necessary for several key thyroid functions. This deficiency will impact thyroid and possibly pituitary function causing what appears to be a thyroid condition when in reality it is a fixable problem that can restore normal thyroid function without the need for thyroid medication(s).
Impact of Genetics
Genetics can play an important part in identifying potential hereditary conditions, such as hypothyroidism, and potential T4 to T3 conversion issues. While these will have impacts on treatment(s), which I’ll cover in the next article, it is essential to know if you fall into either of these categories during your diagnosis.
Thyroid function and homeostasis involve the use of three different deiodinase enzymes: deiodinase 1 (D1), deiodinase 2 (D2) and deiodinase 3 (D3). (3) Here is a brief overview of each deiodinase enzyme:
- Primarily found in the liver, kidney, and thyroid gland the D1 enzyme is responsible for facilitating the conversion of T4 into the active T3 thyroid hormone.
- Primarily found in the brain, pituitary gland, skeletal muscle, and brown adipose tissue, the D2 enzyme facilitates the conversion of T4 to T3 at the intracellular level for regulating processes like brain development, the hypothalamus-pituitary-thyroid (HPT) axis, and any intracellular needs of the body.
- Located throughout the body’s tissues, the D3 enzyme facilitates the inactivation of the T3 hormone by cleaving off one iodine atom turning it into T2. (Scientists used to think T2 was an inactive hormone but the latest science shows T2 is actually an active hormone that primarily helps T3 with metabolic regulation.) The D3 enzyme can also take T4 and create rT3, which signals to the cells to slow down metabolic activity as a result of disease, surgery or serious injury or illness.
Each of the deiodinase enzymes has a corresponding gene that could influence any of the thyroid conditions. The D1 enzyme is associated with the DIO1 gene; the D2 enzyme with the DIO2 gene; and the D3 enzyme with the DIO3 gene. You inherit one allele, part of the makeup of the gene, from each parent. If one of the alleles is bad from one of your parents, you have a heterozygous mutation. If you receive two bad alleles, one from each parent, you have a homozygous mutation.
Mutations in any of the genes, specifically the DIO1 and DIO2 genes, can cause dysregulation of the enzyme(s) to do their job. A heterozygous mutation may cause slight T4 to T3 conversion issues while a homozygous mutation will severely impede this conversion making it necessary to supplement with T3 medication or even be a T3-only patient if you cannot produce enough T3 from the conversions within the body.
It is becoming more common for medical professionals to order genetic tests to look at potential thyroid gene mutations if they suspect you could have genetic reasons for T4 to T3 conversion issues.
Atrophic Thyroiditis
Atrophic thyroiditis is one of the rarer autoimmune thyroid conditions that can be extremely difficult to diagnosis. It can be a very slow acting or rapidly moving condition that can manifests over a lifetime or as short as a month. There may or may not be any permanent damage to your thyroid, which is why this condition may show present in tests one time and not in subsequent tests. It can also be present with either Hashimoto’s or Graves diseases or neither of them.
The essence of this condition, and the only real tell-tale sign of its presence, is the overall shrinkage or atrophying of the thyroid gland. However, some people experience shrinkage but no atrophy. Non-congenital thyroid atrophy is caused by TSH-receptor *blocking* antibodies (TBAb – Thyroid Blocking Antibodies), a variant of Graves’ disease TSHR (Thyroid Stimulating Hormone Receptor) *stimulating* TSAb (Thyroid Stimulating Antibodies). The TBAb and TSAb can coexist and complete with other. (4)

As you can see:
- It is difficult to test for and detect unless you measure and compare total thyroid volume sizes over time.
- It can co-exist alongside the other autoimmune conditions (Hashimoto’s and Graves’) making it difficult to parse one condition from another.
- There can be little to no progression and take quite a bit of time to manifest.
- Both blocking and stimulating antibodies can be present at the same time, essentially balancing your thyroid activity behind the scenes.
Atrophic Thyroiditis can cause a misdiagnosis as it can either incite or block a hypothyroid or hyperthyroid condition. Careful review of labs and symptomology is necessary to rule this autoimmune condition in or out.
Goiters, Nodules and Cancers
Goiters
A goiter is the enlargement of the thyroid gland due to a critical deficiency or sustained inflammation of the gland. It may not be visible unless it is allowed to grow and then could become quite large causing both physical problems, such as pressure pain, breathing issues, difficulty swallowing, coughing, and thyroid hormone dysfunction. One of the main causes of a goiter is iodine deficiency. However, it can also evolve from a nodule or one of the autoimmune conditions (Graves or Hashimoto’s).
A goiter can interrupt the adequate production of thyroid hormones thus appearing to cause hypothyroidism or hyperthyroidism. You may be able to correct this hormone dysfunction if the goiter is detected early and treated. This may include iodine treatment if found to be deficient. Surgery, thyroid medication, or radiation may be an option but these are rarer options. As long as there is no thyroid dysfunction or physical impairments your doctor may choose to monitor its growth until surgery may become necessary.
Nodules
A nodule(s) is relatively common, especially in the aging population with women having a greater occurrence than men. The majority of thyroid nodules are benign, with 5% to 15% being malignant. (5) Nodules are normally abnormal growths of thyroid tissue that grow out of the thyroid gland and vary in shape and size. However, sometimes they can be fluid-filled like a cyst, which may pop and disappear on its own.
Nodules can be present for years without notice or can interfere with thyroid function. You can have one or more nodules located on either lobe or on the isthmus, the connecting section of the two lobes. The way nodules interfere with thyroid function is by causing disruption in hormone production thereby producing either hypothyroid or hyperthyroid symptoms. You may not actually have either condition but the nodule(s) may mimic them.
Nodules can grow in size and may become palpable. They may also grow large enough to interfere with vocal chords, voice harshness, and exert pressure on the esophagus or trachea creating problems breathing and eating. There are surgical and radiation means to treat them but they often are ineffective in shrinking, removing all offending tissue, and restoring full thyroid function. Most nodules, usually greater than 1cm in size, are measured and monitored every six to twelve months for abnormal growth in shape and size until action may be required.
Your Endocrinologist may decide to do a Fine Needle Aspiration (FNA) biopsy if an ultrasound or CT Scan indicates abnormalities in any of the nodules or surrounding lymph nodes. Your doctor will then evaluate the biopsy results, your scans, palpable results and your symptoms to help determine if any of the nodules have traits of malignancy or are negatively impacting your neck health. This is based on their tool called TI-RADS (Thyroid Imaging Reporting and Data System), which calculates a score evaluating five categories of traits. Depending on your TI-RADS score, and if a definitive finding of malignancy from the FNA is found, surgery may be required to remove one lobe or the entire gland in order to remove the offending tissue.
Thyroid Cancers
The thyroid gland has several kinds of cells that can grow cancer: follicular, C cells, lymphocytes and stomal cells. There are four main types of cancers that can develop in the thyroid gland, usually within nodules or goiters but can grow out of the thyroid cells too. The four cancers are papillary, follicular, medullary and anaplastic. Papillary cancer is the most common type and found in 80% of patients with cancer. (6)
Thyroid cancer can physically damage the gland itself, which disrupts hormone production. Cancer can also negatively affect nodules and goiters by causing them to enlarge and impinge on surrounding neck structures. It can also spread to surrounding lymph nodes and become metastatic. Some of these cancers grow slowly, sometimes over years, and some grow fairly quickly and can spread outside the gland.
Suspicious nodules or goiters seen in an ultrasound or CT Scan may cause your Endocrinologist to order a FNA to gather thyroid material for further testing. Results can return positive for malignancy, negative if benign, or indeterminant. Outside a positive FNA result, your doctor will use the scans, symptoms (if any present) and FNA results to evaluate your TI-RADS score to help determine the likelihood of malignancy despite a benign or indeterminant result. (A FNA can only grab a small amount of material from an area of tissue where the malignancy may not be present yet. Most times your doctor will gather at least two samples from different areas of the tissue, nodule or goiter from greater accuracy.)
Treatment of thyroid cancers depends on the type and stage. It can range from watching for further changes in thyroid gland operations up to a thyroidectomy, the removal of the entire thyroid gland. (The parathyroid glands are relocated in the neck if they are healthy.) Some elect a lobectomy, the removal of the infected half of the thyroid gland, while others choose radiation therapy to kill the infected nodule(s), goiter or thyroid tissues. Others may need chemotherapy if cancer becomes metastatic. Some may need a combination of therapies. (7)
Most likely any cancers or cancer treatments will negatively impact thyroid hormone function. This would require treatment with thyroid medications perhaps until healed or maybe even for life.
Thyroid and Lipedema Diseases: Life Out of Balance – Part 2 Summary
Diagnosing a thyroid condition or disease can be both scary and relieving to receive validation all the symptoms you’ve been experiencing is actually a genuine problem(s) that needs attention. Making the diagnosis requires reviewing 1) ALL your thyroid panel tests, 2) ALL your supportive vitamin and minerals tests, 3) documentation of your symptoms, 4) a review of family history, and 5) any genetic factors that may influence thyroid functions. All of these allow your doctor to make an accurate diagnosis.
Making a thyroid diagnosis may be straightforward. However, careful attention needs to be paid to extenuating circumstances that may mimic a thyroid condition but actually turn out to be an essential vitamin or mineral deficiency that impacts thyroid function. This may also be the case with the presence of nodules, goiters and cancers which can impact thyroid function. There is also an elusive autoimmune condition, called atrophic thyroiditis, that can negatively impact thyroid function directly or exist alongside one of the other autoimmune thyroid diseases.
Properly diagnosing your condition(s) will guide your treatment regimen. This may include watching and waiting for changes, resolving a vitamin or mineral deficiency, performing selective radiation or chemo therapies, surgery, or thyroid hormone supplementation. We will explore that in our next thyroid care segment.
Remember, you are a partner with your Endocrinologist or Naturopath striving to restore your quality of health. Together you will need to make the best decisions on accepting a diagnosis(es) and establishing a treatment plan you can support. Ask plenty of questions until you feel comfortable with the plan.
Stay tuned for the third part of the thyroid life of out of balance series where we’ll discuss treatment options for thyroid conditions and diseases.
My Personal Story: Hypothyroidism, and perhaps Hashimoto’s, runs in my maternal family but I was unable to connect the dots until two years ago at age 60. Did you know there is a relationship between serious viral infections, particularly Epstein-Barr Virus (EBV), and the development or exacerbation of Hashimoto’s? My mother and I both had our initial EBV infection in our 50s, which is very late in life, with occasional flares of the virus. It is possible this virus and the flares exacerbated our Hashimoto’s condition and we never knew it. Unfortunately, both of us had elevated TPO Antibodies and all the symptoms of Hashimoto’s but were denied a diagnosis. We were told our antibody levels, while elevated, were not high enough for a diagnosis. The doctors also did not support the concept of autoimmune-based thyroid conditions. My mother suffered with serious hypothyroidism symptoms up until her death in 2020. I refused to allow that to happen to me and finally found a Naturopath who supported the severe hypothyroid diagnosis and began immediate treatment this year. We are waiting for my genetic results to see if I have any of the DIOx mutations, which may explain my T4 my T3 conversion issues. I will update when I learn more.
Stay tuned —> Thyroid and Lipedema Diseases: Life Out of Balance – Part 3 where I discuss thyroid treatment options
To Your Improved health!
References:
- (1) Dr. Westin Childs – New Optimal Thyroid Lab Ranges for All Thyroid Lab Tests
- (2) National Institute of Health: National Library of Medicine – Effect of Micronutrients on Thyroid Parameters
- (3) National Library of Medicine: National Center for Biotechnology Information – Deiodinases and the Three Types of Thyroid Hormone Deiodination Reactions
- (4) Thyroid Patients Canada – The Spectrum of Thyroid Autoimmunity
- (5) National Library of Medicine: National Center for Biotechnology Information – Thyroid Nodule Size and Prediction of Cancer: A Study at Tertiary Care Hospital in Saudi Arabia
- (6) American Cancer Society – What Is Thyroid Cancer?
- (7) American Cancer Society – Treatment of Thyroid Cancer, by Type and Stage
Resources:
- National Library of Medicine: National Center for Biotechnology Information – The relationship between thyroid disorders and vitamin A.: A narrative minireview
- Paul Robinson – Could Atrophic Thyroiditis Be Your Problem? It is Not Always About Hashimoto’s Thyroiditis
- National Library of Medicine: National Center for Biotechnology Information – Prevalent Polymorphism in Thyroid Hormone-Activating Enzyme Leaves a Genetic Fingerprint That Underlies Associated Clinical Syndromes
- National Library of Medicine: National Center for Biotechnology Information – Pathophysiological relevance of deiodinase polymorphism

