Thyroid and Lipedema Diseases: Life Out of Balance – Part 3
As we discussed in the previous article, life is about balance. When your life or your body is out of balance it opens the door to disease and chronic conditions, among those are thyroid conditions and diseases. Unfortunately, the prevalence of thyroid conditions is rapidly on the rise and if you are experiencing any of the symptoms listed in the previous articles (Part 1 and Part 2) then you should strongly consider having your thyroid function fully evaluated by an Endocrinologist or a qualified Naturopath.
Once you have your diagnosis from your Endocrinologist or Naturopath (aka Functional Medicine doctor or Integrative Medicine doctor) and you concur on the findings, the next step is designing a treatment plan. Treatments can vary depending on your diagnosis and you also have options within those treatments.
This article will explain the most common type of treatments by condition. We will explore non-medicine options, hormone replacement therapies and surgical options as well as handling potential hormonal impacts on future life events.
Remember, you are a partner with your doctor and need to fully understand what is making you feel sick and the treatments that will work to restore your health. Educate yourself the best you can so you can have meaningful conversations about treatment options and how to move forward on the best path possible. Both of you are trying to achieve the same thing – your improved health!
Treatment Options – Non-Medicine Based
Watch and Wait Option
When is this option used?
This option usually applies to non-malignant nodules and goiters, sometimes known as tumors, that are not currently interrupting thyroid hormone production or causing symptoms. This active surveillance therapy may involve regular ultrasounds or fine needle aspirations (FNAs) to monitor for any changes in size, shape or characteristics that may indicate a more serious condition. If tumors grow to larger than 0.3mm, spread to surrounding lymph nodes, or start impinging on trachea, esophagus or vocal chords making it difficult to swallow, breathe or talk without a raspy voice then surgery or other treatment options may be considered.
What is the treatment?
This is the easiest treatment option and usually applies to early detection of a non-malignant nodule(s) or goiter. Your doctor will take preliminary measurements and FNAs as a baseline and schedule you for follow-up tests to see if the size, shape or aspects of the nodule(s) or goiter has changed.
You may go months or years in a watch and wait state. However, whenever the size, shape or other aspects change your doctor may decide to take further action to treat your condition. Depending on the severity of the changes they could recommend:
- Hormone supplementation if your hormones levels have changed
- an ablation procedure
- a lobectomy (removal of half of your thyroid gland)
- an isthmusectomy (removal of the isthmus area of your thyroid gland) or
- a total thyroidectomy (removal of the entire thyroid gland)
Depending on the nature of the changes in your condition you will be presented treatment options. Sometimes, as in the advanced cancers, medullary or anaplastic, you may have limited options.
Ablation
When is this option used?
This treatment is usually used in an attempt to shrink growing or impinging nodules and goiters caused by a hyperthyroid condition or eradicate two of the four kinds of thyroid cancers (papillary and follicular).
What is the treatment?
Ablation is a non-surgical destructive process used to shrink symptomatic nodules and goiters. There are two types of ablation your doctor may use to try and shrink your nodules. The first is radiofrequency ablation (RFA). It uses targeted radio waves to heat up and burn the affected nodules. Nodules that are solid or mostly solid, cause impingements in the neck area, are cosmetically visible or cause overproduction of hormones (hyperthyroid condition) are the best candidates for RFA.
RFA is done on an outpatient basis, usually under a mild sedative, and causes minimal discomfort. Doctors will use an ultrasound to guide the process and accurately target each nodule. Reduction of the nodule(s) may take up to a month to confirm and occasionally patients may need to repeat the process to continue current nodule reduction or address subsequent nodules. It is the safer of the two ablations and unlike a surgical solution does not leave a scar.
The second type of ablation is called radioactive iodine (RAI). It is normally done for those with hyperthyroid nodules or certain types of cancers (papillary or follicular). Your thyroid requires iodine to make hormones. In RAI your thyroid uptakes special iodine that is radioactive, that targets and kills just your thyroid cells. The iodine-131 is available as oral capsules, an oral drinking solution and IV injections. Depending on your dose the RAI can take effect anywhere between 3 and 14 days. You will need to isolate yourself from other people during this time as you will emit a low level of radiation. This process essentially kills your entire thyroid gland without surgically removing it. You will need to discuss this option with your doctor to decide if this process is the best one for your needs. (1)
There are other types of ablations, including laser, cryo (freezing), ethanol and radioactive remnant, but RFA and RAI are the two most common ones used to address nodules, goiters and affected thyroid tissue.
Radioactive Remnant Ablation (RRA) is a special type of ablation used in post-thyroidectomy cancer patients when thyroid tissue remnants are detected and need to be destroyed. Sometimes RRA is used in conjunction with RAI to kill off any remaining tissues, especially tissue that is infected with cancer. Your doctor will decide which radioactive treatment(s) are necessary depending on the size, amount of and type of cancer detected in your body. (2)
Treatment Options – Medicines

There are essentially two types of thyroid medications used in hormone regulation. First, there are synthetic versions that treat either the T4 or the T3 hormones, but are separately administered and monitored. Second, there is NDT (Natural Desiccated Thyroid), which is the whole natural ground up porcine thyroid gland and contains both T4 and T3 hormones.
Synthetic Medication
Pros: This is the most common type of medication and is usually lower in cost. It also allows your treating medical professional to decide which hormone solution is right for your condition and carefully control the dosage of each one. You may only need T4 (mono-therapy) or you may need both T4 and T3 (dual therapy) medications for regulation. Many people do well on mono or dual therapy. However, some people experience T4 to T3 conversion issues and all their T4 hormone can do is essentially make reverse T3 (rT3) instead of the active T3 hormone. This may necessitate them moving to a T3-only mono-therapy.
Cons: Some people do not tolerate synthetic medications. They may have digestive issues, reactions to fillers or dyes, or more serious symptoms that necessitate changing to another synthetic version or even choosing a NDT.
Synthetic T4 Hormone Options (USA)
- Levothyroxine (Sodium) (generic)
- Synthroid
- Levoxyl
- Novathyrox
- Unithroid
- Tirosint (gel cap for those with digestive troubles)
Synthetic T4 Hormone Options (Outside USA)
- Thyronorm
- Eltroxin
- Thyrox
- Euthyrox
- Thyrofit
- Lethyrox
- Vencamil
- Oroxine
- Eutroxsig
- Levoxine
Synthetic T3 Hormone Options (USA)
- Liothyronine (generic) (slow release or regular)
- Cytomel (slow release or regular)
Synthetic T3 Hormone Options (Outside USA)
- Thyonin
- Tertroxin
- Linorma T
- Thybon 20 Henning
Natural Desiccated Thyroid (NDT) Medication
Pros: It has been used since the late 1800s for the treatment of hypothyroidism, so it has been well tolerated for a long time. People with sensitivities to synthetic medications usually find relief in using a NDT. The ratio of T4 to T3 is well proportioned as it contains the entire contents of the porcine thyroid gland. If you need both T4 and T3 medications, this might be an acceptable option for you. It should also be noted that some people use a NDT with a synthetic T3 medication if they require additional active hormone.
Cons: The FDA (Food and Drug Administration) regulates the porcine version of the NDT. If you have allergies to porcine meat you may not tolerate a NDT. NDTs are measured in grains (instead of micrograms) so dosage is less accurate. There is a bovine version of NDT but it is NOT regulated by the FDA. It is sold over the counter and should not be considered unless discussed with your medical provider.
NDT Medications (USA) *
- Armour Thyroid
- NP Thyroid
NDT Medications (Outside USA)
- Armour Thyroid
- ERFA Thyroid (Canadian brand)
- Nature-Throid
- NP Thyroid
- WP Thyroid
**Special note: On August 6, 2025, the U.S. Food and Drug Administration (FDA) announced that it plans to take enforcement action against unapproved animal-derived thyroid medications, commonly known as Natural Desiccated Thyroid (NDT) or Desiccated Thyroid Extract (DTE). The FDA classified these products as unapproved biologics, requiring manufacturers to obtain a Biologics License Application (BLA) to legally market them. The FDA cited concerns over the safety, purity, and potency of DTE products, noting that they are made from animal tissue (pigs) and have not undergone the rigorous approval process required for modern drugs. The FDA is allowing 12 months (until August 2026) for patients and providers to transition to FDA-approved thyroid hormone replacement therapies (such as levothyroxine or liothyronine). It should be noted if the FDA drops its license on the NDTs your medical insurance will probably not cover its costs, so it is important to many patients to carefully watch how things develop later this year.
Thyroid Hormone Dosing
This is a complicated computation with many factors that may take weeks or months to fine tune. Any change in dosing or medication type will take about six to eight weeks to fully register in your system. That’s how long it takes your body to fully adjust to the new dosage(s). In other words, pack your patience when fine tuning your hormone levels.
There is no “one size fits all” formula when setting your initial dose. Many doctors may still base your dosage(s) on TSH levels, but there are several other factors to consider when setting your dosage(s).
Factors to Consider in Dosing
- Age
- Weight
- Severity of symptoms
- Metabolism status
- Current (non-thyroid) medications (some interfere with thyroid medications)
- Stress levels
- Inflammation levels
Advanced Factors Affecting Dosing and Adjustments
- Genetics
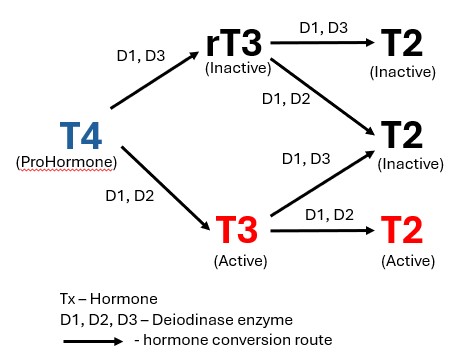
- Ability to process one or more deiodionase thyroid enzymes (D1, D2 and D3) (conversion issues)
- T4 or T3 Hormone sensitivities
- Any gut or absorption issues (SIBO/SIFO)
- Reverse T3 Thyroid Syndrome
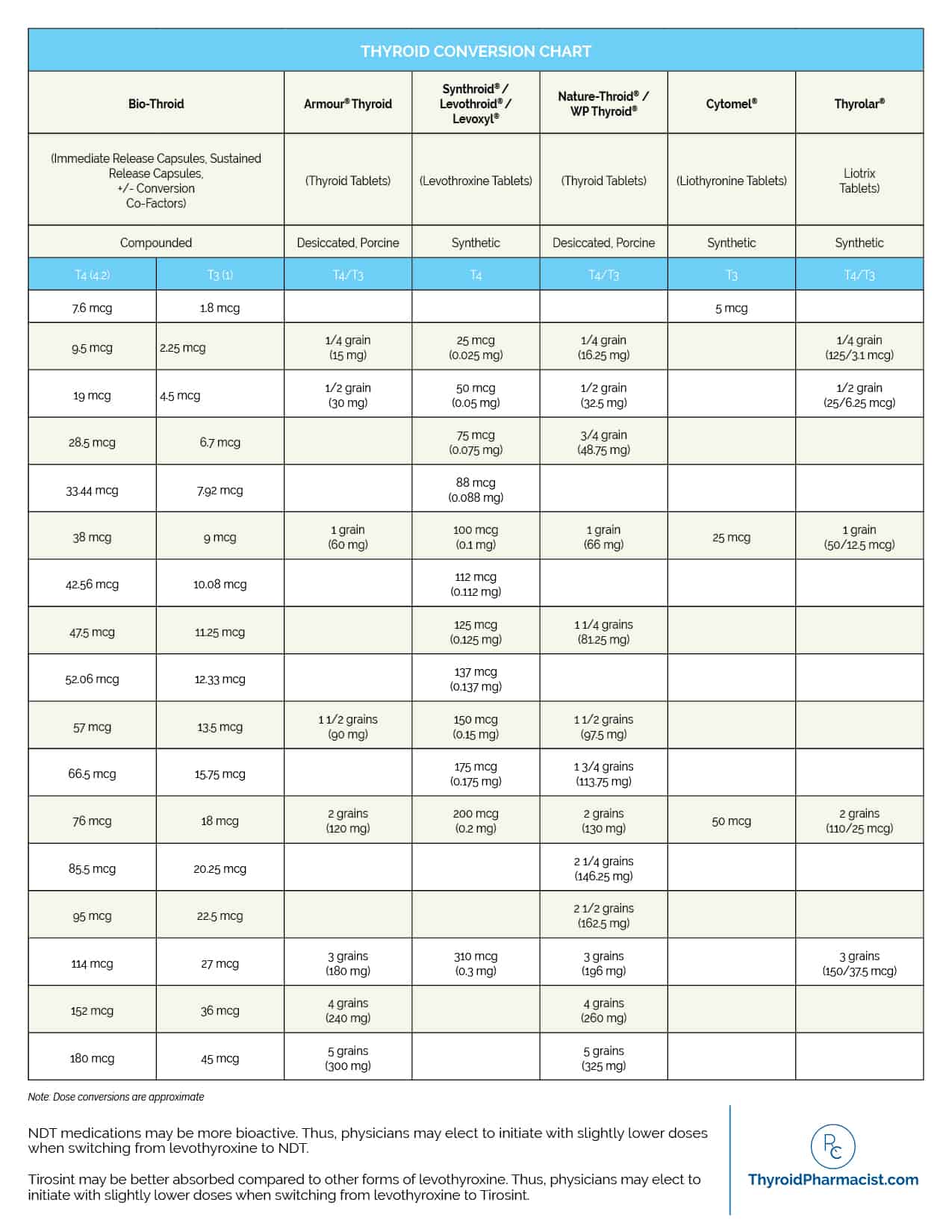
Below is a conversion chart of synthetic medications and NDT medications for reference if you plan to change your medication.
Medication Adjustments
You will need to run your FULL thyroid panel to see how the current dose of medication(s) are affecting your TSH, T4, T3 and rT3 levels. In theory taking the correct level of T4 AND assuming your deiodinase enzymes are working as intended, you should be converting enough T3 to meet your system’s needs.
If you are on a mono-therapy then you may need to adjust your T4 up or down to get your T3 levels in the desired upper one third of the range and produce little to no rT3 levels. If you are on dual-therapy you may only need to adjust your T3 medication to sustain the correct level of this hormone. Running labs every six to eight weeks is vital each time you make a dosage change.
There are more complex situations where your system is having problems converting T4 to T3, usually through a problem with deiodinase enzyme activation. This may necessitate your medical professional to recommend reducing your T4 dose (relying less on its conversion activity) and increasing your T3 dose so that you can have more active hormone in your system. In some cases it may be more beneficial to be on a T3 mono-therapy.
In another situation called Reverse T3 Thyroid Syndrome your T4 is mostly making the rT3 hormone, which essentially hinders the binding and use of the active T3 hormone. If your T4 medication is making mostly rT3 it will be beneficial to be on T3 mono-therapy.
You will notice during these adjustment periods you may start to feel better. Your symptoms will start to improve. However, if you feel little to no change in symptoms you will need to make further changes in either your T4 or T3 medication(s).
Moving Forward With Your Thyroid Medication Treatments
Once you are on thyroid medication(s) and stabilized, it is not a “set it and forget it” event. You will need to continuously monitor your symptoms and call your doctor if symptoms return or complications develop.
Any major life changes can trigger hormonal fluctuations, particularly in your T3 and rT3 hormones, For instance, a major surgery or surgeries within a short period of time that involve anesthesia, infections, ICU (intensive care unit) stays, and any complications can trigger your body to go into “healing mode”. Your body recognizes you don’t need high levels of energy for fat burning but need to conserve that energy for healing. This allows rT3 to “put on the brakes” in your system by taking up receptor sites in your cells so that T3 cannot occupy them. This ultimately lowers your T3 levels, which triggers your hypothyroid symptoms.
Another event that can influence changes in your hormone levels would be significant weight loss. If one of your goals is to start losing weight now that your hormones are balanced, know that at some level of fat loss your body may believe you are heading into “famine mode”. Again, your body uses the rT3 hormone in the same way as healing mode to “put on the brakes” in your system in an attempt to conserve energy. Your T3 hormone levels will drop until your body no longer detects you are in famine mode. You will again start experiencing hypothyroid symptoms.
In both scenarios you will need to see your doctor for assessment and remediation. Remediation may entail increasing your daily T3 hormone and may even reduce your T4 to slow or stop the production of rT3. Remember that any changes to your thyroid hormones takes time, so be patient during the adjustments.
Treatment Options – Surgical
There are several reasons your doctor may recommend a surgical solution to treat your thyroid condition. Those include:
- one or more nodules that are greater than 0.4mm in size, especially if they are impinging on your trachea, esophagus or vocal chords
- Uncontrolled hyperthyroidism that does not respond to any other treatments
- Graves disease where medications are contraindicated
- Fluid-filled cysts that keep returning after being repeatedly drained
- FNAs that return a positive biopsy or high suspicion of malignancy
There are several types of surgeries to treat your specific condition that you and your doctor will discuss. Surgeries should not be entered into lightly as the effect is permanent. Your thyroid gland does NOT regenerate and thyroid transplants are very rare.
Depending on your specific surgery, one, two, three or all four of your parathyroid glands, located on the back of your thyroid gland, will be removed from the gland and relocated to the fatty areas of your neck. The glands that are removed will go into “shock” and may stop functioning for a week or more while it adjusts. You will be given calcium supplementation to keep your calcium levels stable until the glands recover.
Surgery Options
Let’s explore the types of surgeries and when they are indicated.
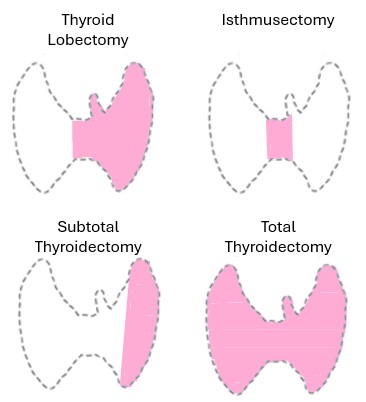
- Isthmusectomy – removal of the isthmus only, the small band of thyroid tissue that connects the two lobes of your thyroid
- Thyroid Lobectomy or Hemithyroidectomy – the removal of only one lobe which usually includes the isthmus, for benign nodules and low-risk cancers
- Subtotal or Near-Total Thyroidectomy – removal of most of the thyroid gland leaving a small amount of thyroid tissue on one side (rare)
- Total Thyroidectomy – removal of the entire thyroid gland usually for large nodules and goiters, Graves disease or specific cancers
- Lymph Node Excision or Lymphadenectomy – removal of adjacent lymph nodes usually performed in confirmed malignancy cases
Barring any complications, your surgery is normally done as a day surgery and you can go home later that day. Sometimes your doctor may decide to keep you in the hospital overnight for observation, especially if there were any complications or drainage issues.
Some people may require a drainage tube in their neck to collect excess fluid from the surgery. It can be removed in as little as a day or may be several days later depending on much fluid and how well you are draining.
Surgeons usually do a good job hiding your incision in the fold of your neck so there is minimal visible scarring. Once your incision is fully healed you can also start using vitamin E cream or other ointments (Mederma or Cicatricure) meant to address scar reduction to minimize the visibility of the scar.
Surgery Medications
All of the surgeries listed above will require some form of hormone supplementation. This may be a T4 mono-therapy or a dual-therapy with T3 hormones. They will have to be balanced with the amount of T4 and T3 the remaining part of your thyroid is producing.
The exception to balancing will be if you have a total thyroidectomy. Your doctor will need to do a total manual balancing effort as there is no contribution from any thyroid tissue. Depending on several circumstances your final therapy may be a mono T4 therapy or a combination of dual therapies with T4 and T3 hormones. In rare case you may end up being on a T3 mono-therapy. See the Treatment Options – Medications section to see what medications you will want to review with your doctor.
My Tips and Tricks
- Do not take your T4 medication (levothyroxine) with coffee and wait at least one hour AFTER taking to eat or drink anything but water.
- Doctors will recommend taking your T4 medication (levothyroxine) in the morning. I take mine at night before bed. It has a sedative effect plus I know I will not be eating right before bed.
- You can take both your T4 (levothyroxine) and your T3 medications together.
- Doctors will tell you to take all your T3 in one dose in the morning. I partition my daily dose into three equal doses and take them 6-8 hours apart. I take my first dose around 5am to help with waking Cortisol levels. This follows your body’s circadian rhythm (see Paul Robson’s article) and sustains your energy and metabolism throughout the day.
Summary of Thyroid and Lipedema Diseases: Life Out of Balance
When life is out of balance it opens the door to disease and chronic conditions. These conditions, particularly thyroid problems, can wreak havoc throughout the body causing issues in other systems. This can include digestive health (stomach, colon, pancreas and gallbladder), insulin management, adrenal health, reproductive health, cardiovascular health, energy production, and lymphatic function to name a few. It can also exacerbate problems in other conditions, such as Lipedema, lymphedema, and obesity already experienced by people in this community.
If you have been diagnosed with a thyroid disease or condition there may be several treatments available to assist in reducing, eliminating or managing your thyroid function. Much will depend on the nature, severity and available options within the treatment path. The easiest treatment is the watch and wait approach, which can last for months or years until a condition progresses. There are non-surgical options such as radioactive iodine, cryo, laser and radiofrequency ablation that can reduce or eradicate thyroid tumors and certain thyroid cancers. There are also several surgical options that may help when tumors impinge on trachea, esophagus or vocal chords or when addressing several types of cancers. They range from partial lobe removal, isthmus removal, entire lobe removal or even removal of the entire thyroid gland.
Outside the watch and wait option the rest of thyroid treatments will require some sort of supplemental hormone medication(s). This could include T4 or T3 synthetic medications, or natural desiccated thyroid medications. The type and dosage levels will be determined by how much your thyroid gland is producing on its own unless you’ve had a total thyroidectomy and then you will be wholly reliant on full T4 and possibly T3 medications.
Once you establish your new optimal thyroid hormone levels you should be good for a while. However, remember that major life events, such as traumas, surgeries or large weight loss amounts, can trigger a change in your thyroid hormone levels and your hypothyroid symptoms may return. This may require you to reset your hormone levels to compensate. Please talk with your Endocrinologist, Thyroidologist or Naturopath about any return of hypothyroid symptoms for possible hormone dosage changes or possible medication reactions.
My Personal Story: Hypothyroidism runs in my maternal family but I was unable to connect the dots until two years ago at age 60. I had several nodules on both lobes and the isthmus, one of them pressing against my trachea and esophagus. In 2021 one nodule tested 90% malignant and I had to make a very difficult decision (especially during the COVID pandemic) on treatment. In October 2021 I had a total thyroidectomy with pathology showing papillary cancer in nodules not previously tested, several additional large nodules and undiagnosed Hashimoto’s disease. I have lived on both T4 and T3 medications for the last 4.5 years due to T4 to T3 conversion. In 2025 I had to switch to a Naturopath with Endocrinology training due to medication limitations of my Endocrinologist. We have been rebalancing my thyroid hormones but encountered problems with two difficult surgeries and a SIBO (small intestinal bacterial overgrowth) imbalance (caused by my severe hypothyroidism in 2024). Now (January 2026) I am experiencing a huge shift in my thyroid hormones due to the collective trauma of my surgeries (associated anesthesia, complications, persistent bacteria infections and over 13 doses of antibiotics) over these past six months and a 100+ pound weight loss over the last year (2025). My body thinks I am in “famine mode” and “healing mode” so it is using rT3 to stop my metabolism and drop my T3 levels below range. Unfortunately, this has reactivated my SIBO (as it requires T3 to stay in remission) so it is very messy right now. I will also note I do have the genetic mutations for the DIO1 and DIO2 deiodinase enzymes, which lends creditability to my conversion issues. Even with all these challenges, the rebalancing is making a HUGE difference in my quality of life!
Missed an Episode —> Thyroid and Lipedema Diseases: Life Out of Balance – Part 1 where I discuss the thyroid, its function, necessary tests and prevalence in Lipedema women and Part 2 where I discuss how to diagnose thyroid disease and conditions
To Your Improved Health!
References:
- (1) Cleveland Clinic – Radioactive Iodine Therapy
- (2) National Library of Medicine – National Center for Biotechnology Information – Radioiodine Remnant Ablation: A Critical Review
- (3) Thyroid Pharmacist – Medications for Hashimoto’s and Hypothyroidism
Resources:
- University of Washington – Radiofrequency Ablation (RFA) for Thyroid Nodules
- Springer Naure: BMC Endocrine Disorders – Evaluating the effectiveness of combined T4 and T3 therapy or desiccated thyroid versus T4 monotherapy in hypothyroidism: a systematic review and meta-analysis
- Recovering with T3: My Journey from Hypothyroidism to Good Health using the T3 Thyroid Hormone (Recovering from Hypothyroidism) (Book 1) – Paul Robinson
- The CT3M Handbook: More on the Circadian T3 Method and Cortisol (Recovering from Hypothyroidism) (Book 2) – Paul Robinson
- The Thyroid Patient’s Manual: From Hypothyroidism to Good Health (Recovering from Hypothyroidism) *Book 3)- Paul Robinson
- The Thyroid Fix: Reduce Fatigue, Lose Weight, and Get Your Life Back – Dr. Shawn Soszka
- Stop the Thyroid Madness: A Patient Revolution Against Decades of Inferior Treatment – Janie Bowthorpe
- The Thyroid Connection: Why You Feel Tired, Brain-Fogged, and Overweight — and How to Get Your Life Back – Amy Myers

Surgery With Lipedema

Thyroid and Lipedema Diseases: Life Out of Balance – Part 2
