SIBO: Complications – Part 2
SIBO Complications
- SIBO Complications
- Malabsorption / Nutritional Deficiencies
- Malnutrition
- Migrating Motor Complex (MMC)
- Exocrine Pancreatic Insufficiency (EPI)
- Bile Acid Malabsorption (BAM)
- Structural
- Kidney Stones
- Mast Cell Activation Syndrome (MCAS)
- Glucagon-like Peptide-1 Receptor Agonists (GLP-1s)
- Pathogens, Inflammation and Lymphatics
- Blood Clots
- SIBO: Complications – Part 2 Summary
There are many conditions in other body organs and systems that can be affected by a SIBO imbalance and vice versa. Some can be severe and possibly permanent if not recognized and treated quickly. We will explore some of the more common complications that occur with SIBO and what you can do to mitigate or repair them.
Malabsorption / Nutritional Deficiencies
The SIBO bad bacteria metabolize nutrients (specifically fats, carbohydrates, and key vitamins and minerals) before the body can absorb them. If SIBO continues untreated it can lead to unwanted weight loss, nutritional deficiencies, and, in severe cases, damage to the intestinal lining. Some of the malabsorption issues experienced include:
- Fat malabsorption – bacteria affects the structure of bile, which in turn impairs fat absorption causing steatorrhea (fatty, foul-smelling stools). Without adequate fat transport mechanisms your body cannot properly utilize fat-soluble vitamins thus creating deficiencies. These include vitamin A, D, E and K and any other vitamins taken in liposomal format.
- Vitamin B12 deficiency – unfortunately the bad bacteria consume vitamin B12 faster than the body can, thus creating a B12 deficiency. This may require regular injections, tablets, patches or sublingual options to maintain adequate levels until the SIBO can be healed.
- Iron Deficiency and Anemia – iron is another common mineral grabbed first by the bad bacteria before the body can absorb it. A deficiency in iron causes a lack of healthy red blood cells that is required to carry oxygen to all cells in the body. This can lead to anemia, which causes fatigue, pale skin, shortness of breath, dizziness and colds hands and feet. Remediation requires iron supplementation, infusions or transfusions if severe.
- Carbohydrate malabsorption – This occurs when the small intestine cannot digest sugars and starches, passing them into the colon where they ferment. This will cause bloating, gas, diarrhea, and fatigue.
If malabsorption issues and nutritional deficiencies are not treated promptly you will start experiencing malnutrition issues, which can be quite harmful to the body, and in some cases even fatal. It is imperative to identify and treat your SIBO and underlying root cause to avoid these serious complications.
Malnutrition
If malabsorption and nutritional deficiencies continue to degrade over time without proper treatment, malnutrition will develop. This is a serious condition which can negatively affect other body organs and systems and can even turn fatal if not immediately remediated. Symptoms of malnutrition include:
- Severe digestive distress (increased bloating, gas, cramping, abdominal pain and diarrhea)
- Unintentional and rapid weight loss (severe nutritional deficiencies particularly in B12, iron and calcium)
- Severe fatigue and weakness (chronic fatigue, muscle weakness and general unwellness)
- Stool changes (stool that has oily appearance, smells strong and floats due to fat malabsorption)
- Neurologic issues (brain fog, moodiness, confusion, headaches)
- Bone health (osteopenia or osteoporosis due to poor calcium absorption)
- Skin and hair issues (hair loss, rashes and dry skin due to severe deficiencies)
SIBO malnutrition treatment involves identifying and resolving the root cause of the SIBO. However, in the short term you may need intramuscular injections of key vitamins and minerals for a while until your body is able to start absorbing them again. This is particularly important for the fat soluble vitamins (A, D, E, K and vitamin B12). Digestive enzymes may also be required at every meal to help with digestion and absorption issues, particularly fat absorption.
You will need to be under the care of your doctor to monitor your progress and adjust treatment as necessary.
Migrating Motor Complex (MMC)
Gastrointestinal motility refers to the ability to move food from your mouth all the way through the digestive tract and out of the body through the anus. This is accomplished by one-way muscle contractions (peristalsis) that operate in a wave-like pattern.
Under normal circumstances motility flows in one direction. However, certain conditions can cause impaired motility causing a backwash of food and fluid that can be harmful to your system. It is commonly seen in acid reflux (GERD), esophageal spasms (dysphagia), trouble emptying stomach content into the small intestine (gastroparesis), and trouble moving content through the intestinal tract. Other impairments can interfere with motility which include abdominal surgery abnormalities, hernias, diverticulitis, bariatric surgeries as well as medical conditions like diabetes, infections and certain medications.
The MMC is a special type of mobility that works on the small intestine essentially “sweeping” residual bacteria. food particles and other pathogens into the colon where it can be properly processed and disposed. When the MMC stops working bad bacteria, such as with SIBO, is allowed to grow and spread. If you have a leaky gut it can also allow these endotoxins, pathogens and food particles to escape into the blood stream usually triggering an immune response and further infections.
The MMC requires about a three hour window to do its complete sweep, so it is important to finish your meal and not eat (no snacking or grazing) for at least three to four hours. This is an essential function of healing your SIBO by preventing the backward flow of the bad bacteria from the colon into the small intestine. Every effort needs to be made to restart the MMC and promote its continued function for SIBO healing and a healthy digestive tract.
There are several conditions that impact the function of the MMC. These include hypothyroidism, diabetes, stress, the use of GLP-1 medications, and nervous system interruptions from the gut-brain axis via the vagus nerve operation to name a few. Correcting these conditions can help heal and restore normal MMC function. Read more about MMC operations and impacts to your motility.
Exocrine Pancreatic Insufficiency (EPI)
SIBO and EPI have a bi-directional relationship often exacerbating both conditions. There is a high prevalence of people with EPI also testing positive for SIBO and vice versa. SIBO can interfere with the pancreas’ ability to release digestive enzymes, which include lipase, amylase, and protease. These enzymes are responsible for the digestion of the protein, fat and carbohydrate macronutrients in your system. Without these critical enzymes, undigested food is consumed by the bad SIBO bacteria, quickly passes out of your system, and may even exit the small intestine and enter the bloodstream.
Some people with SIBO and EPI may have chronic pancreatitis, which produces similar symptoms to SIBO. If chronic pancreatitis exists it may permanently affect the pancreas’ ability to make adequate digestive enzymes even after SIBO is healed. However, many people who have co-occurring conditions of SIBO and EPI may have full recovery of both conditions once healing is achieved.
EPI is diagnosed primarily through stool tests, with the Fecal Elastase-1 (FE-1) test being the most common. The 72-Hour Fecal Fat Test is the gold standard for measuring fat malabsorption, involving a special diet and three-day stool collection to detect excessive fat in the stool (steatorrhea). Your doctor may also use imaging or blood tests to check for any scarring or fibrosis of the pancreas as well as the presence of any nutritional deficiencies that impact exocrine function.
If your levels are too low you will need to supplement your pancreas activity by taking digestive enzymes, known as PERTS (pancreas enzyme replacement therapy) until your pancreas can heal. PERTS are taken with every meal to aid in digestion. The most commonly prescribed PERTS are:
- Creon – most commonly prescribed capsule that comes in varied doses
- Zenpep – another commonly prescribed capsule
- Pancreaze: coated capsules or microtablets
- Pertzye: known for smaller particle sizes.
- Viokace – only tablet form usually paired with a proton pump inhibitor (PPI)
Digestive enzymes are sold over the counter but note they may not be strong enough to aid in digestion. Most people with chronic pancreatitis or SIBO-induced EPI usually take the stronger prescription medications. You may be able to eventually stop taking digestive enzymes once your SIBO and EPI are healed.
Bile Acid Malabsorption (BAM)
SIBO often causes a bile acid malabsorption condition by breaking down (deconjugating) bile salts, which leads to fat malabsorption, chronic diarrhea, and nutrient deficiencies. This improper fat digestion issue causes mucosal damage accompanied by fatty, greasy stools (steatorrhea), bloating, and weight loss. The unabsorbed bile acids quickly enter the colon where they irritate the intestinal lining and are quickly excreted by the system instead of bile being reabsorbed into the body. You will notice your diarrhea will be medium to bright yellow from the excess bile.
BAM, especially when combined with SIBO, lowers B12 levels (bad bacteria consumes it first) thus creating a well-documented metabolic phenomenon known as the “methyl-folate trap” or the “high-folate–low-vitamin B12 interaction”. B12 and folate (B9) have an inverse relationship so as B12 levels lower folate levels rise. Folate requires B12 to be converted into its active form for use in the body. Without sufficient B12, folate becomes “trapped” in a form (5-methyl-tetrahydrofolate) that cannot be used effectively by cells. Since the body cannot use the “trapped” version of folate, blood work will show high levels of folate and conversely make B12 levels look much lower.
The challenge with this scenario is the high folate can essentially mask the B12 anemia, potentially causing damage thus allowing continued neurological symptoms (numbness, tingling, cognitive decline), which could potentially become irreversible. Your doctor can verify this condition via blood work by testing your blood looking for low B12, high folate, high methylmalonic acid (MMA), and high homocysteine levels. Your doctor may also look for genetic mutations in the MTHFR (MethyleneTetraHydroFolate Reductase enzyme) genes that impact both B12 and folate methylation and treat accordingly.
Treating BAM with SIBO is a two-pronged effort both involving diarrhea reduction. BAM treatment uses a binder (sequestrants) to stop the bile acids from irritating the colon lining. Examples of binders include Cholestyramine, Colestipol, and Colesevelam. A low-fat diet is also recommended to reduce the need for bile needed for digestion. Consult your doctor for proper dosing as too much can further irritate the colon and increase the diarrhea.
Structural
Structural or anatomical issues in the abdomen can allow food stagnation, inflammation and thinning of the intestinal walls, and obstructions in the successful removal of food particles and bad bacteria. Conditions like Celiac disease, Ehlers Danlos Syndrome (EDS), and Crohn’s disease can influence the structural integrity of the digestive system. Some people may even need a surgery or medical procedure to fix a structural issue before SIBO can fully heal.
Examples of structural or anatomical issues that can help foster the growth of bad bacteria or other medical conditions include:
- Adhesions (scar tissue) – abdominal surgeries may cause small intestine adhesions that can slow motility or create stagnant areas where bacteria or food particles have trouble passing (hernia repairs can also cause scar tissue).
- Ileocecal Valve Dysfunction – a malfunctioning valve, which may be caused by surgery or weakness from underlying tissue fragility and laxity caused by EDS, allows bacteria from the large intestine (colon) to backflow into the small intestine.
- Diverticula – these small pockets located in the intestinal wall can hide food particles and bacteria where they get stuck and are difficult to clear.
- Surgical “Blind Loops” – blind loops occur usually in the stomach and small intestine during a bypass procedure (gastric bypass surgeries, intestinal resections) where the digestive process is bypassed or blocked thus creating stagnation and fostering bacteria growth.
- Strictures and Fistulas – this is a narrowing or unnatural connections in the intestines which can slow down motility creating possible obstructions or areas where bacteria can grow. This is common in those with Crohn’s disease or have abdominal scarring.
- Reduced Motility or Dysmotility – this may not always be caused by structural issues but can alter the structure of the gut wall thus weakening contractions and reducing the effectiveness of the MMC.
Structural or anatomical issues can exacerbate SIBO symptoms and delay healing. Some people may need to address the underlying issue to gain relief of symptoms and be able to move on to healing.
Kidney Stones
SIBO significantly increases the risk of developing kidney stones, particularly calcium oxalate stones which are the most common, due to fat malabsorption and increased intestinal absorption of oxalate. SIBO causes fat malabsorption, allowing an increased binding of calcium to fat in the intestine, leaving excessive free oxalate to be absorbed and excreted in urine or stored in the kidney..
Normally, calcium binds to an oxalate in the digestive tract allowing it to be removed from the system. However, without adequate available calcium to bind to the oxalate enters the bloodstream eventually being processed or stored in the kidney, increasing the chances of forming stones. This is particularly concerning if you have a history of kidney stones or a family history of stones.
“The microbiome plays a key role in the formation, recurrence and treatment of kidney stones. The microbiome profiles of healthy and stone-forming patients differ significantly, with a reduction in oxalate-degrading organisms and an enrichment of pathogenic organisms being the central hallmarks. The microbiome influences stone formation through metabolic regulation, inflammatory response, and alteration of the urinary microenvironment, particularly through the ‘gut-kidney axis’. Intervention strategies targeting the microbiome (e.g., probiotics, metabolite modulation) provide new ideas to reduce stone risk.” (1)
Mast Cell Activation Syndrome (MCAS)
For those that have Mast Cell Activation Syndrome (MCAS), SIBO can be a vicious bidirectional cycle. MCAS triggers inflammation thus reducing motility. This in turn causes more bacterial overgrowth. SIBO then continues to produce additional endotoxins and pathogens which keep the mast cells in a hyperreactive state.
Unfortunately, MCAS can cause symptoms of bloating, abdominal pain and diarrhea (impaired motility), which mimics those of SIBO. It can also cause nausea and vomiting with gastrointestinal conditions. Anaphylaxis is the worst symptom of MCAS, which can affect your respiratory and cardiac systems. There are several levels of anaphylaxis, the most severe usually requiring the use of an EPI pen and treatment in the emergency room or even fatality.
“The relationship between SIBO and MCAS is as follows; SIBO causes activation of mast cells and increase in T lymphocytes. T lymphocytes in turn secrete microparticles that again activate mast cells. Activated mast cells and T lymphocytes release cytokines that increase intestinal permeability[37]. This leads to a vicious cycle in which intestinal permeability is constantly impaired and inflammation is constantly increased[36,38].” (2)
If you suffer with MCAS along with your SIBO you may need to treat as needed with MCAS stabilizers. Some take daily medications to regulate mast cell responses, which can include H1 antihistamines such as cetirizine (Zyrtec), fexofenadine (Allegra), or loratadine (Claritin) and H2 blockers, which include famotidine (Pepcid) or cimetidine (Tagamet). For more serious reactions some may need to take Benadryl as a rescue medication. Others may need stronger stabilizers such as cromolyn sodium and ketotifen, which require a prescription from your doctor.
Some may also need to supplement with a Diamine Oxidase (DAO) enzyme to help mitigate histamine foods and reactions, especially when battling SIBO. SIBO damages the gut lining, decreasing the level of DAO enzyme, which is necessary for the breakdown of histamine, thus increasing the histamine response. Supplementation may be another tool to use to mitigate the MCAS response.
Glucagon-like Peptide-1 Receptor Agonists (GLP-1s)
GLP-1s are a class of medications usually prescribed to those with type 2 diabetes, weight management issues and obesity to help address blood sugar management and weight loss efforts. GLP-1s are meant to mimic the effects of the body’s natural GLP-1 hormone that is released after eating.
Its primary purpose is to regulate insulin release and reduce glucagon release when blood sugar levels are high. It also slows down the motility of the digestive system, forcing food to move more slowly from the stomach into the small intestine and then into the colon. This signals the brain to promote feelings of fullness and less hunger.
The digestive system operates in a sequential contraction wave motion from your mouth all the way to your anus. This rhythmic motion, especially through the intestinal tract, needs to remain constant to avoid the likelihood of overgrowth development or bowel obstructions, which can lead to debilitating conditions. It may also interfere with the critical operation of the MMC, which keeps your small intestine clean, not to mention disrupting the balance of your gut microbiome. When you forcibly change the design of this rhythmic pattern you will be increasing the risk of opening the door to conditions like SIBO, IBS, IMO (Intestinal Methanogenic Overgrowth) and ISO (Intestinal Sulfide Overproduction). You will also be slowing down the circulatory and lymphatic movements as they rely on the established motility of your digestive tract.
Those who take GLP-1s may not see any changes to their bowel patterns right away. Sometimes, motility issues can take three, six, nine or twelve months to manifest. Monitor yourself for symptoms and consult your medical professional if you experience any of the SIBO symptoms. More studies are being conducted on the effects of GLP-1s on the digestive system, but preliminary studies are showing up to 30% of GLP-1 users showing positive test results for SIBO. (3)
There are other dietary factors to consider when assessing the risk of developing overgrowth conditions. Negative impacts to eating habits can hasten motility problems while positive changes can lessen the effects of an overgrowth condition or even help prevent the development of the condition. These changes include:
- Nutritional quality of daily meals (balanced macronutrients)
- Grazing and snacking habits
- Caloric changes (reduction or significant increase)
- Nutritional deficiencies
- Supplements and medications taken daily
Before considering a GLP-1 regimen, review the causes section of SIBO (and other overgrowth conditions) to assess your risk of motility issues. If you have one or more of the defined listed risk, please review the situation with your medical professional as a GLP-1 solution may not be right for you. Certainly those with current IBS, SIBO, dysbiosis, gastroparesis, Ehlers Danlos Syndrome or other motility issues should strongly evaluate their fitness to weather the potential of motility issues caused by GLP-1 use.
Pathogens, Inflammation and Lymphatics
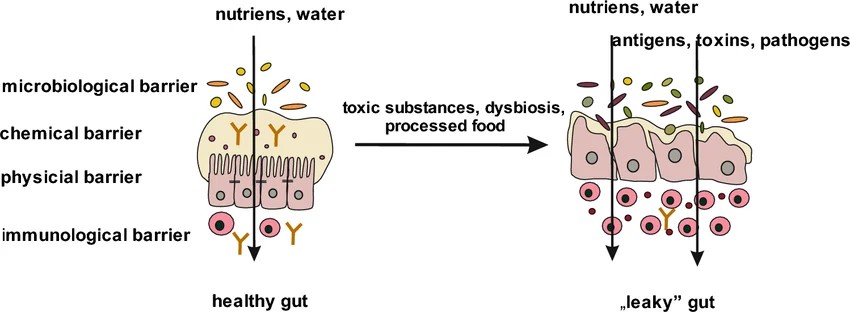
Approximately 70–80% of your immune system resides in your gut, making it the front line for identification and clearance of pathogens. (4) In people with “normal” healthy digestive systems, the gut barrier helps maintain homeostasis. In people with infectious disease, overgrowths, lymphatic dysfunction, and dysbiosis the gut works overtime to mitigate pathogens, fight inflammation, promote digestion, and restore motility.
These four basic barrier layers allow the absorption of essential nutrients, water and electrolytes while also providing protection for any microorganism anomalies it encounters.
- Microbiota layer (lumen) – the inner hollow space of the intestine which contains commensal (beneficial) bacteria for digestion activities
- Mucus (biochemical) layer – is about 98% water and contains mucins, glycoproteins, IgA antibodies, and antimicrobial substances. The mucus also coats epithelial cells and protects them from the harmful effects of pathogenic microorganisms and toxic substances
- Epithelial layer – which is the physical barrier that consists of a single layer of specialized cells: enterocytes, goblet cells (produce mucins), Paneth cells (produce antimicrobial peptides and proteins), enteroendocrine cells, M cells and intestinal stem cells
- Immune layer – consists of intraepithelial lymphocytes (IELs), Peyer’s patches, which are clustered lymphoid papules, lymphocyte clusters, and gut-associated lymphoid tissue (GALT), which contains antigen-presenting cells (APCs), T lymphocytes, B lymphocytes, plasma cells, as well as macrophages, mast cells and granulocytes. (5)
When any of these layers is compromised, such as with overgrowth conditions, particularly SIBO, it disrupts the function and protection provided by the intestines. SIBO negatively impacts the balance of good and bad bacteria in the small intestine. This causes an increase in pathogens and negatively impacts motility.
If you have a compounding condition, specifically leaky gut (and many people do whether they know it or not), you will have “holes” instead of “tight junctions” in your epithelial layer where pathogens and undigested food particles can exit the intestinal tract. If these particles get through the scrutiny of the immune layer and into the bloodstream it could create a host of problems for the body including:
- Systemic inflammation (including a mast cell response if you have MCAS)
- Infectious disease from one or more pathogens
- Possible development of an autoimmune condition
- Increase the permeability of the intestinal barrier
Your intestinal tract is lined with structures called villi, finger-like protrusions from the wall, that absorb nutrients (sugars, amino acids, and fatty acids), secrete mucus to line the epithelial cells and help pass food, and provide surveillance and mitigate pathogens. Inside each villi is a vein and artery for blood supply and a lymphatic capillary called a lacteal.
The lymphatic structure functions slightly differently than the rest of the body’s lymph structure. Lymph movement in the intestinal tract relies on the standard rhythmic motility that moves food through the entire digestive tract. The small intestine lymph fluid drains into the superior mesenteric lymph nodes while the colon drains into the inferior mesenteric lymph nodes.
When motility is negatively impacted the lymph fluid does not move well and can even become stagnant. This will cause negative impacts to the entire systemic lymph system, creating swelling and pain. Restoring motility as quickly as possible will help alleviate lymphatic impacts, allow for improved nutrient absorption and movement, and aid in mitigating any mounting pathogen problems.
Secondarily, reducing local and systemic inflammation will assist in restoring normal lymphatic function and aid in SIBO healing. Once you have begun working on rectifying these key issues, you may want to investigate a tolerable and effective means of manually moving lymphatic fluid. (You may need to avoid working directly on your gut area during your initial condition development as it may be too painful for your gut.)
You can check out Dr. Perry Nickelston’s Big 6 manual lymph draining program on the MLD web page. Note: it is recommended you start slow and maybe start with step one or the first two steps for a while until you confirm no negative effects to your system. Some may not tolerate a lot of lymphatic movements at first, especially if you have never done drainage or it has been a long time.
Personal Experience: I had undiagnosed and untreated SIBO for 11 months when I unexpectedly ended up in the hospital in July 2025. I had a stuck kidney stone, life-threatening sepsis and a gut full of endotoxins while in the middle of a SIBO detox. After emergency surgery to place a stent for the stone and antibiotic treatment for the sepsis, a couple weeks later I developed a subsequent bacterial infection from the colonization of my stent. It turned out to be the enterococcus faecalis strain and again was back on antibiotics to try and resolve it. In November 2025 I developed sepsis two days before my lithotripsy and had to undergo the procedure and replacement stent with significant risk as part of the cure. Again, the enterococcus faecalis bacteria reappeared and colonized my second stent. I was put on more antibiotics until I was healed enough to finally remove the stent at the end of December.
No one knew where the enterococcus faecalis bacteria came from and now with my SIBO knowledge we might finally have an answer. The enterococcus faecalis bacteria safely lives in your colon and is beneficial to the digestive process as long as it stays within its intended confines. However, when it is released into the small intestinal and escapes the barrier confines, such as in the case with leaky gut (which I have), it can enter the bloodstream (translocates) and become a dangerous bacteria to your system. It is an antibiotic-resistant strain and I had to take a “reserve” potent antibiotic in order to clear the infection. The enterococcus faecalis bacteria can, and probably did, cause my sepsis twice as well. This demonstrates how dangerous SIBO can be, especially when you have “holes” in your intestinal barrier as with leaky gut!
Special note – I tried to put my custom compression garments on just my lower legs for a couple days and ended up exacerbating my SIBO situation. I went back to diarrhea and more than a dozen trips to the bathroom as my gut could NOT handle the extra lymph fluid and toxin movement in my system. So now I have had to stop all additional lymphatic activities until my SIBO is healed and my gut lymphatics are flowing better.
Blood Clots
Clot formation in the venous system usually manifests commonly as deep vein thrombosis (DVT) and pulmonary embolism (PE). In rarer cases, about 1%, these clots can develop in the abdominal region in the mesenteric blood supply area and are known as mesenteric venous thrombosis (MVT). (6) In susceptible veins there is usually damage to the vessel wall, venous stasis and hypercoagulability, which helps define its pathogenesis. DVTs are usually found in the calf or thigh areas while PEs are usually found in the lungs.
There are many reasons a DVT, PE or MVT can form. This can include hereditary factors, particularly in first line relatives. A genetics report may be able to identify those factors. There are also blood tests your Hematologist can run to look for coagulation factors to see if you have the propensity to clot abnormally. In people with SIBO, there is a significant production of pro-inflammatory mediators from the overgrowth of bacteria, which can be a factor in the coagulation of blood. Given the small intestine empties into the superior mesenteric circulatory and lymphatic systems it is not uncommon problems, particularly blood clots, could occur.
When conditions exist for a MVT blood clot, you will start to experience ischemia. Ischemia is a serious condition where reduced blood flow restricts oxygen and nutrients to tissues, which can lead to severe problems including intestinal necrosis. migrating blood clots, obstructions, and even fatality (which is estimated at 50% of cases). (6) Recognizing the symptoms and getting rapid care will determine the severity of your outcome. Symptoms include rapid onset of severe abdominal pain (usually left side), bloating, nausea or vomiting, inability to eat or drink, bloody stool and fever.
Medical professionals can see these clots on a CT Scan along with any potential signs of necrosis. In most cases of MVTs necrosis is present and doctors need to perform an emergency re-sectioning of the bowels to remove the dead and dying tissues. In all cases of one or more MVTs your doctor will place you on a blood thinner to help your body dissolve the clot(s) over time. Usually they will reevaluate your situation in six months to determine if it is safe to stop the anticoagulant or continue longer, especially if any testing shows factors for clotting issues.
In rarer cases, the increased pressure in the portal vein area, commonly referred to as portal hypertension, needs an outlet to shuttle excess blood supply. Here’s where your body does something amazing. Your body can take your umbilical vein (called ligamentum teres after birth), a vein that has not been used since birth and never intended to be used again, and reconstitute it to provide additional blood relief for the portal vein area due to the occluded MVT(s) area. The vein reconstitution or recanalization is more common in patients with liver cirrhosis or cancer that present with portal hypertension but very rare in the case of MVT issue relief absent of liver problems. (7)
There needs to be more studies and research in the connection between SIBO and the formation of venous thrombosis. Venous thrombosis and reconstitution of the umbilical vein outside of a liver cirrhosis situation is poorly understand and most likely under-reported.
Personal Experience: In January 2025 I suddenly started experiencing left-side abdominal pain along with a fever and the inability to eat or even hold water down. I went to the emergency room where they did a CT Scan, which revealed four MVTs in my superior mesenteric area. Thankfully, they did not see any signs of necrosis (which is common if not treated immediately). They did however, see the reconstitution of my umbilical vein as a response to the reduced blood supply to the area. How’s that for adaptive and amazing!
I was immediately admitted and started on heparin. It took several days to achieve the correct dose to effectively manage the blood clots. I was switched to oral anticoagulants, which I took for eight months. A follow-up CT Scan in July showed all the blood clots were gone and I had no cofactors, markers or hereditary factors indicating risks of future clotting issues. So far, so good as we continue to monitor that area since I am currently battling a relapse in my SIBO condition.
SIBO: Complications – Part 2 Summary
As you have just read, SIBO can negatively affect some of the body’s other organs and systems and conversely SIBO can be worsened by other body system complications. Among some of the most damaging complications that need to be closely monitored include malabsorption issues that lead to nutritional deficiencies which can ultimately lead to malnutrition. This situation can damage other organs and even be fatal if not promptly corrected.
Healing your SIBO overgrowth and restoring the normal operation of the small intestine requires a functional MMC. If the MMC is not working, the small food particles and pathogens infesting the small intestine cannot be “swept” away into the colon for proper disposal. This also involves a dietary and meal spacing change to reactivate this critical housekeeping function. Other measures may need to be made to correct the root cause of SIBO and MMC dysfunction.
The pancreas has a bi-directional affect with SIBO. It can be a cause of SIBO or pancreatic exocrine functions can be affected by a SIBO situation. Either way, you may end up treating both conditions by taking digestive enzymes to aid in absorption problems until both conditions are healed.
The gallbladder secretes bile to aid in the breakdown of food in the small intestine. As it moves through the colon on its way to the exit the bile is reabsorbed by the system and stored back in the gallbladder for future use. However, when you have persistent diarrhea the system empties too quick purging the bile with it. This will lower your B12 levels and artificially raise your folate levels. You may need to rebalance the B12 and folate levels until BAM and SIBO are healed.
Structural or anatomical issues in the abdomen can allow food stagnation, inflammation and thinning of the intestinal walls, and obstructions while trying to remove food particles and bad bacteria. Conditions like Celiac disease, Ehlers Danlos Syndrome (EDS), and Crohn’s disease can influence the structural integrity of the digestive system. Some people may even need a surgery or medical procedure to fix a structural issue before SIBO can fully heal.
SIBO absorbs many of the minerals and vitamins as soon as they enter the small intestine, which includes calcium. Calcium binds with the loose oxalates in your gut so it can be safely flushed out of your system. Non-bound oxalates end up landing in your kidneys where they sit and bind with other loose oxalates creating potential kidney stones.
MCAS is another bi-directional problem for those with SIBO. SIBO causes inflammation, which over activates your mast cells (for those with MCAS) causing additional inflammation and negative symptoms in your body. If the small intestine is seriously compromised it may not be able to produce enough DAO enzyme, which breaks down histamine, and will cause a complex repeating condition.
GLP-1 use is a controversial topic as it is marketed for weight loss, insulin management and inflammation reduction. The main action of GLP-1s is to mimic the effects of the body’s natural GLP-1 hormone and to slow down motility thus making you feel satiated longer. This can have a negative impact on those with any motility issues, currently including those with SIBO, other overgrowths, IBS, Celiac disease, Crohn’s, gastroparesis, and gastric bypass to name a few. Careful consideration needs to be exercised when considering adopting its use.
Your small intestine will experience a slowing of motility with SIBO that makes moving blood supply and lymph extremely slow or even stagnant. This inhibits critical nutrient absorption and pathogen mitigation. A leaky gut can exacerbate the issue by releasing dangerous pathogens into the bloodstream and creating serious systemic infections. If you pump or use compression wraps you may need to stop until SIBO is healed to prevent forced lymph movement through an already compromised area and introducing additional toxins into an area rife with them.
Blood clots are not an uncommon condition and studies are starting to show the inflammatory materials produced by SIBO can contribute to venous thrombosis. It is more common to experience DVTs in the calves and thighs or PEs in the lungs. However, since small intestine drainage happens in the superior mesenteric area it is now supported SIBO can also contribute to MVTs in the abdomen, which can cause severe repercussions in the intestines or even be fatal.
It is important to be aware of all these conditions and to promptly address any issues that impact SIBO healing or your system as a whole. Many of these complications have permanent or dire outcomes that may be preventable with early detection and treatment. My hope is that you do not experience any of them as SIBO can be challenging enough to tackle, but awareness is key to keeping your system moving in a healing direction.
Stay tuned for —> SIBO: Treatments and How to Know When You’re Healing – Part 3 and review SIBO: Definition, Symptoms, Diagnosis, Causes and Related Conditions – Part 1.
To Your Improved Health!
References:
- National Library of Medicine – How is the human microbiome linked to kidney stones?
- National Library of Medicine – Mast cell activation syndrome: An up-to-date review of literature
- National Library of Medicine (PubMed) – Diagnostic Evaluation of an Increased Risk of Developing Small Intestinal Bacterial Overgrowth Associated with Glucagon-like Peptide-1 (GLP-1) Receptor Agonists and Dual GLP-1/GIP Receptor Agonists: A Global Retrospective Multicenter Cohort Analysis
- National Library of Medicine (PubMed) – The Interplay between the Gut Microbiome and the Immune System in the Context of Infectious Diseases throughout Life and the Role of Nutrition in Optimizing Treatment Strategies
- ResearchGate (Clinical and Experimental Medicine) – Intestinal permeability disturbances: causes, diseases and therapy
- National Library of Medicine (PubMed) – Intestinal Obstruction as Initial Presentation of Idiopathic Portal and Mesenteric Venous Thrombosis: Diagnosis, Management, and Literature Review
- ScienceDirect (Journal of Vascular Surgery: Venous and Lymphatic Disorders) – Mesenteric vein thrombosis can be safely treated with anticoagulation but is associated with significant sequelae of portal hypertension
Resources:
- TrioSmartHealth.com – Demystifying the Types of SIBO, Symptoms, Causes, Testing, & Treatment Options
- Dr. Westin Childs – 8-Step SIBO Protocol: Diet, Treatment, Supplements & more
- Association between hypothyroidism and small intestinal bacterial overgrowth – PubMed
- [Thyroid-intestinal motility interactions summary] – PubMed
- National Library of Medicine – Small Intestinal Bacterial Overgrowth
- National Library of Medicine – Gut microbiota in patients with kidney stones: a systematic review and meta-analysis
- TrioSmartHealth.com – Your GLP-1 Might Be Affecting Your Gut More Than You Think
- Sage Journals – GLP-1 Receptor Agonist Use Is Associated With Small Intestinal Bacterial Overgrowth and Intestinal Methanogen Overgrowth
- Philadelphia College of Osteopathic Medicine – Safety, Benefits and Side Effects of GLP-1 Weight Loss Medications
- Rupa Health – A Functional Medicine SIBO Protocol: Testing and Treatment
- MastCell360.com – What is SIFO? Is it a Mast Cell Trigger like Mold?
- National Library of Medicine (PubMed) – Recanalization of port-superior mesenteric vein thrombosis with long-term anticoagulant therapy after failed early anticoagulant therapy
- National Library of Medicine (PubMed) – Association between small intestinal bacterial overgrowth and deep vein thrombosis
- American Journal of Gastroenterology – Small Intestinal Bacterial Overgrowth Increases the Risk for Deep Vein Thrombosis

SIBO: Treatment and How to Know if You’re Healing – Part 3

SIBO: Definition, Symptoms, Diagnosis, Causes and Related Conditions – Part 1
